1951
We talk frequently about the H5N1 virus mutating to a form transmissible between humans, although we acknowledge we don't know the factors that make that transmissibility possible. There is also the possibility that the virus, if mutated, will modify its current virulence. The case fatality rate (proportion) now is hovering around an extremely high 50%. However we don't understand the factors that affect these factors in any influenza sub-type, including the current seasonal variety, H3N2. Even within the yearly H3N2 seasons there is a four-fold variation in mortality.
We are now realizing that in some years there are extraordinary mortalities that exceed those seen in pandemics, including the pandemic of 1918. Our relative ignorance about these variations is emphasized dramatically in a fascinating paper in CDC's Emerging Infectious Disease journal by NIH's Cecile Viboud and her co-authors.
Viboud et al. detail a new investigation of the 1951 H1N1 epidemic:
The results are striking:
We are now realizing that in some years there are extraordinary mortalities that exceed those seen in pandemics, including the pandemic of 1918. Our relative ignorance about these variations is emphasized dramatically in a fascinating paper in CDC's Emerging Infectious Disease journal by NIH's Cecile Viboud and her co-authors.
Viboud et al. detail a new investigation of the 1951 H1N1 epidemic:
Anecdotal accounts exist in the literature of historical influenza epidemics associated with unusual numbers of deaths, such as occurred in the 1951 epidemic in England in the midst of the first era of A/H1N1 viruses (1918–1957). In Liverpool, where the epidemic was said to originate, it was "the cause of the highest weekly death toll, apart from aerial bombardment, in the city's vital statistics records, since the great cholera epidemic of 1849". This weekly death toll even surpassed that of the 1918 influenza pandemic. (Viboud et al.; all cites omitted)The authors compiled monthly pneumonia and influenza (P&I) and all-cause death numbers between 1950 and 1999 in Canada, England and Wales and the US and used additional data for Liverpool where the disease seemed particularly severe. Using the monthly data they fit seasonal variation in a 20 year span to be able to compare the 1951 epidemic with the 1957 and 1968 events, controlling for differences in population, healthcare and socioeconomic status, all factors that affect P&I deaths (age-adjustment and mortality in the summer of 1960 were used to adjust the seasonal estimates for this purpose). A shift toward younger age groups was used as a pandemic signature.
The results are striking:
Influenza activity started to increase in Liverpool, England, in late December 1950. The weekly death rate reached a peak in mid-January 1951 that was ≈40% higher than the peak of the 1918–19 pandemic, reflecting a rapid and unprecedented increase in deaths, which lasted for ≈5 weeks (see figure). Since the early 20th century, the geographic spread of influenza could be followed across England from the weekly influenza mortality statistics in the country's largest cities, which represented half of the British population. During January 1951, the epidemic spread within 2 to 3 weeks from Liverpool throughout the rest of the country.
For Canada, the first report of influenza illness came the third week of January from Grand Falls, Newfoundland. Within a week, the epidemic had reached the eastern provinces, and influenza subsequently spread rapidly westward.
For the United States, substantial increases in influenza illness and excess deaths were reported in New England from February to April 1951, at a level unprecedented since the severe 1943-44 influenza season. Much milder epidemics occurred later in the spring elsewhere in the country.
Local disparities were found in all 3 countries, with a consistent pattern of higher numbers of deaths in locations affected earlier. In England, influenza-related death rates were ≈3-fold higher in Liverpool than in the rest of the country. In Canada, death rates were ≈2.4-fold higher in the eastern seaboard provinces than in the rest of the country. Similarly, in the United States, rates were ≈2.3-fold higher in New England than in the rest of the country.
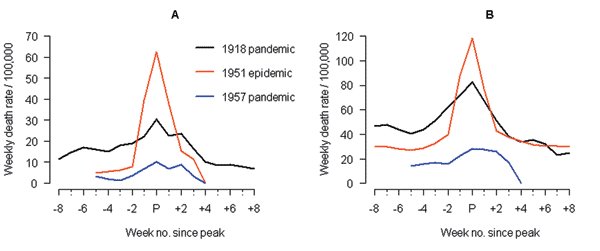 Figure 1 from Viboud et al. paper: Liverpool P&I deaths (A) and all cause deaths (B)
Figure 1 from Viboud et al. paper: Liverpool P&I deaths (A) and all cause deaths (B)In Canada this was the most severe influenza epidemic in the second half of the 20th century, including both pandemic years of 1957 and 1968, by a factor of 50% and 200 - 300%, respectively. Similar results were seen in England and Wales. In the US, by contrast, the flu season was mild, except in New England.
The suspicion that England and Wales and Canada may have experienced an epidemic with a novel sub-type was not confirmed by an examination of the age distribution, which was typical of interpandemic years. 1957 and 1968, by contrast, did exhibit the age shift thought to be a characteristic pandemic signature. The Canadian data for 1951, the only one where detailed age breakdowns were available, showed that the death rate in the younger age groups was almost as high as in the 1957 pandemic, but the death rate in the over 65 age group was double that of the 1957 pandemic. Thus the age distribution wasn't shifted to the younger age groups but markedly increased across the age groups. Additional analyses suggested it was not transmissibility that characterized the 1951 outbreak but the virulence of the virus, although data are not sufficient to establish this with certainty. The subtype circulating at the time was H1N1, the same subtype as the 1918 pandemic and the predominant seasonal form until the H2N2 pandemic of 1957.
But what about the markedly lower death rate in the US (except for New England)?
These disparities are in part explained by laboratory surveillance reports by WHO, indicating that 2 antigenically distinct influenza A/H1N1 strains cocirculated in the Northern Hemisphere during the 1951 epidemic. The so-called "Scandinavian strain" was isolated in northern Europe and associated with mild illnesses. By contrast, the "Liverpool strain" was associated with severe illnesses and high deaths in Great Britain, Canada, southern Europe, and Mediterranean countries . As both strains cocirculated in some countries, intrasubtypic cross-immunity might have existed, with these 2 strains competing for susceptible hosts.No viral isolates or genetic sequences are available for the 1951 virus, so the source of the unusual virulence of the Liverpool strain remains unknown. This intriguing paper underlines once again how much we don't know. The elderly seemed to do relatively well in the pandemics of 1957 and 1968, but suffered disproportionately in the non-pandemic year of 1951 where they did worse than in two of the three 20th century pandemics in England, Wales and Canada and worse in Liverpool than in any pandemic, including 1918.
A well-known flu researcher said to me recently he thought he knew more about flu 20 years ago than he does now. With the publication of this paper, we might say we also know less about seasonal influenza now than we did last month.
posted by Revere at
4/07/2006 07:19:00 AM
![]()
![]()

<< Home